





Historically, ovarian cancer is often diagnosed at advanced stages because of vague symptoms and presentation, but with new advancements in diagnosis and treatment options, patients with the disease are living longer than ever.
Treatment options for ovarian cancer include local and systemic therapies. Surgery is often the main treatment focus for ovarian cancer with staging and debulking (removing as much disease as possible) as a primary goal. Systemic therapies, such as chemotherapy, may be recommended neoadjuvantly (before surgery) or adjuvantly. Chemotherapy may also be administered intraperitoneally (injected directly into the abdominal cavity). Most patients with ovarian cancer require additional treatment after first-line therapy because of high incidence of recurrence.
Researchers are studying ways to improve identification of risk factors, early detection strategies, chemotherapy combinations, and targeted therapies to address individual pathogenic drivers behind cancer development.
Late and Long-Term Effects
Survivorship care that incorporates disease status, quality-of-life concerns, side effects, and coordination of care is critical at all levels of treatment—active or maintenance, survivorship surveillance, or palliative care.
Treatment- or disease-related side effects vary in severity and impact on quality of life. Long-term fatigue is one of the most common side effects, and it may be exacerbated by other effects such as insomnia, anemia, nausea or vomiting, anorexia, and pain. Patients may struggle with body image, distress, anxiety, depression, fatigue, or other symptoms.
Sexual side effects include loss of libido, vaginal dryness, dyspareunia, and treatment-related menopause after surgery or chemotherapy. Nurses must routinely evaluate for those symptoms because patients may not bring them up. Management strategies include vaginal moisturizers, water-soluble lubricants, use of a vaginal dilator, or referral to sexual health specialists.
Bowel and urinary changes such as diarrhea, constipation, strictures, bowel obstructions, urinary frequency, and urgency may occur from either the disease or treatment and have a significant effect on patients’ quality of life. Interventions depend on the etiology.
Ascites and tumor-related pain can be managed with early palliative care, including paracentesis and pain management. Peripheral neuropathy is usually related to taxanes and platinum agents; pharmacologic interventions such as duloxetine can help manage painful neuropathy, and patients whose feet are affected should be evaluated for fall risk.
Myelosuppression risk increases as treatment becomes more aggressive or repeated. Targeted agents (e.g., bevacizumab and other antiangiogenesis drugs) can cause hypertension, bleeding, poor wound healing, fistulas, and perforations. PARP inhibitors such as olaparib, rucaparib, and niraprib, which are most often used for BRCA1 and BRCA2 variants, are associated with fatigue, myelosuppression, nausea, vomiting, and diarrhea. Patients may require an intraperitoneal catheter or central venous catheter to allow for administration of antineoplastics which require appropriate follow-up and maintenance care.
Refer patients to psychosocial support and psychological counseling for distress from loss of fertility, body image changes, fear of recurrence, anxiety, and depression. Mindfulness and active participation in care may help patients manage feelings of uncertainty.
Ongoing Screening and Prevention
Although many patients achieve initial complete responses from first-line therapies, recurrence risk is high. An appropriate surveillance plan includes close follow-up, history, and physical examination to evaluate for local or distant recurrence, biomarker monitoring with CA-125 levels, and radiologic imaging. Oncology nurses can coordinate care among the interprofessional team, including radiation, surgical and gynecologic oncology, medical oncology, and other specialties to optimize disease surveillance and reduce duplication of studies.
For long-term survivors, focus on disease prevention and screening for second or secondary cancers. To facilitate continuity of care during the transition to primary care, share information such as a treatment summary, individualized survivorship treatment plan, and evidence-based guidelines for surveillance.
Sample Ovarian Cancer Survivorship Care Plan
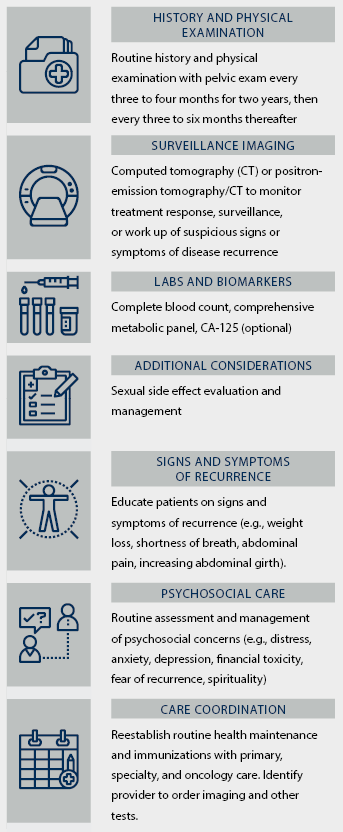
Note. Based on information from the American Cancer Society, National Comprehensive Cancer Network, and Salani et al.