





By Clara Beaver, MSN, RN, AOCNS®, ACNS, BC
In 2021, approximately 44,000 people will be diagnosed with thyroid cancer, most commonly younger patients and assigned females at birth.
Thyroid cancer has three main types: differentiated (e.g., papillary, follicular, Hurthle cell), medullary, and anaplastic. Thyroid lymphomas, thyroid sarcomas, parathyroid cancers, and other rare tumors account for less than 4% of all thyroid cancers. Most types can be treated successfully, with five-year survival rates averaging 98%.
Survivorship care plans are particularly important for this population. Organizations such as ACS, the American Society of Clinical Oncology, and the National Comprehensive Cancer Network have evidence-based guidelines for disease management that include supportive and survivorship care.
Late and Long-Term Effects
Surgery, consisting of a lobectomy or thyroidectomy with or without lymph node removal, is the main treatment for all thyroid cancers except anaplastic. Some patients may receive radioactive iodine to ablate any remaining thyroid tissue not removed during surgery or to treat any other areas where the cancer may have spread. All patients who have had their thyroids removed will begin thyroid hormone therapy to help maintain the body’s metabolism and potentially prevent recurrence.
Patients who have medullary or anaplastic thyroid cancer, experience recurrence, or have metastatic disease often receive external-beam radiation therapy. Chemotherapy is rarely used as primary treatment, but it may be used in combination with external-beam radiation for patients with anaplastic thyroid cancer. It also has a role in advanced cancers that are no longer responding to other treatments.
Targeted therapies are under investigation for thyroid cancers, and findings suggest their utility in patients with papillary or follicular cancers that did not respond to surgery and radioactive iodine therapy. Medullary and anaplastic thyroid cancers do not often respond to thyroid hormone–based treatment, but targeted therapies have shown some benefit.
Most patients with thyroid cancer will have had their thyroids removed or destroyed by treatment. The most common long-term side effects of surgery include dysphagia, dysphonia, and transient or permanent hypocalcemia. For patients who have received radioactive iodine the most common long-term side effects reported are dry eyes (xerophthalmia) and dry mouth (xerostomia).
Fear of recurrence and secondary cancers are also common in this patient population, especially for those diagnosed at a young age. Patients have also reported experiencing anxiety, depression, and fatigue following treatment.
Sample Thyroid Cancer Survivorship Care Plan
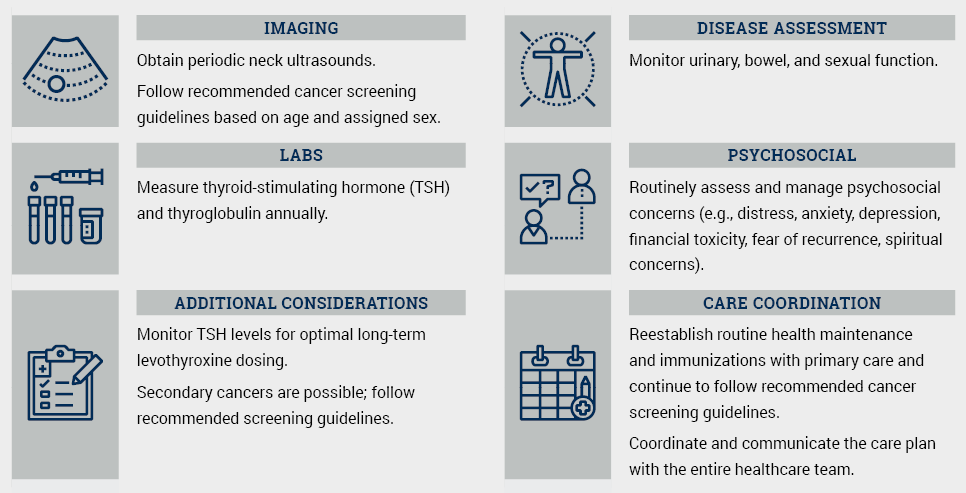
Note. Based on information from American Cancer Society and National Comprehensive Cancer Network.
Ongoing Screening and Prevention
Thyroid cancer survivors will need to be followed by a primary care physician after treatment, especially if their thyroid was removed and they are on thyroid hormone therapy to ensure their hormones are kept at the appropriate level. Patients should follow ACS recommendations for decreasing their cancer risk, including avoiding tobacco, maintaining a healthy body weight, being physically active, consuming a healthy diet, and avoiding or limiting alcohol intake. Risk-reduction recommendations should be included in all survivorship care plans for patients with thyroid cancer. Cancer survivors generally should follow the recommended cancer screening guidelines such as and for their age and assigned sex, including routine colonoscopy, mammography, and other screening recommendations.