





As the use of oxaliplatin in the treatment of gastrointestinal, gynecologic, and other cancers continues to grow, so too does the incidence of hypersensitivity reactions (HSRs) connected to the drug. Because the development of HSRs may require patients to discontinue oxaliplatin even if it’s effective against their cancer, oncology nurses need to be able to prevent or minimize reactions whenever possible.
In their article in the February 2019 issue of the Clinical Journal of Oncology Nursing, Rogers et al. gave an overview of how to prevent, recognize, and manage HSRs from oxaliplatin so that patients have the best chance of continuing successful treatment.
Oxaliplatin HSRs
Oxaliplatin is associated with several toxicities, including peripheral sensory neuropathy, cytopenias, gastrointestinal toxicity, fatigue, and HSRs. Incidence rates for HSRs have been reported to vary from 2%–25%, and some study reports indicated HSR-related treatment discontinuation rates of 21%. The risk of grade 3–4 reactions is about 1.6% and life-threatening reactions is about 1%.
Rogers et al. explained that HSRs typically result from an immunoglobulin E (IgE)/mast cell-mediated action and that symptoms can involve cutaneous, respiratory, cardiovascular, and other systems. (See sidebar for a list of specific symptoms.) Cutaneous symptoms occur in about 45% of HSRs, respiratory in about 42%, and cardiovascular/anaphylaxis rarely.
Because they are IgE mediated, oxaliplatin HSRs occur only after repeated exposure to the drug. Rogers et al. reported that the reactions usually manifest during the seventh to ninth infusion, but some studies cite two peaks in the third and sixth cycle. Additionally, HSR risk increases if patients experience an oxaliplatin-free interval and then are re-exposed to the drug.
Risk factors include female gender, pre-existing allergies to other drugs, lactate dehydrogenase level, and higher neutrophil count but lower monocyte count (for grade 3–4 reactions).
Strategies to Manage HSRs
Prevention is the preferred strategy, Rogers et al. said. Premedications should include antiemetics (e.g., 5-HT3 antagonist with dexamethasone), histamine blockers (i.e., H1 and H2), and corticosteroids. Some studies have shown that intense premedication regimens with high-dose dexamethasone are associated with a lower incidence of HSRs and that they increase the median number of oxaliplatin cycles from 9 to 12.
Treatment choices will vary depending on an HSR’s severity but could include stopping oxaliplatin infusion and administering corticosteroids, histamine blockers, IV normal saline, and oxygen. For severe anaphylaxis, quickly administering epinephrine is critical. Infusion nurses should be prepared to administer those medications, assemble emergency equipment if needed, and assess vital signs every two to five minutes until patients are stabilized.
Resuming Oxaliplatin After HSRs
Although some study reports indicate that oxaliplatin can be resumed the same day if HSRs are mild, most practices will not rechallenge patients on the same day, Rogers et al. said. If HSRs are significant, prescribing physicians should determine whether patients can be rechallenged. However, studies show that oxaliplatin rechallenges are less successful than with other drugs: 50% of patients receiving platinum compounds will experience another HSR despite premedication.
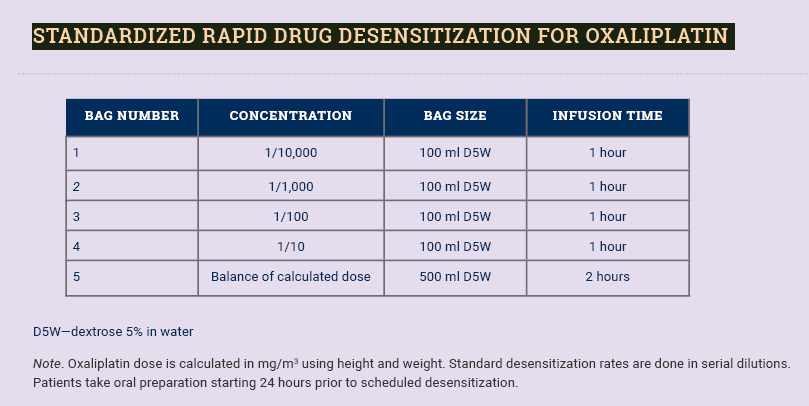
In the case of grade 1–2 HSRs, a rapid drug desensitization (RDD) procedure may enable patients to temporarily tolerate oxaliplatin. Using a predetermined protocol, nurses administer sequentially increasing doses of the drug until the therapeutic amount is reached. Typically, the protocol uses dexamethasone premedication followed by high-dose dexamethasone plus histamine (H1 and H2) blockade. See sidebar for a standardized RDD for oxaliplatin. Because the desensitization is transient, RDD must be followed for every subsequent oxaliplatin administration.
One tool that may help providers decide which patients are most appropriate for a rechallenge is skin testing (e.g., patch, prick, intradermal) to determine mast cell reactivity. Negative skin test results indicate that HSRs are non-IgE mediated and RDDs will be less effective. Researchers reported sensitivity rates ranging from 26%–100%, with patch tests being least specific but prick and intradermal tests producing more reliable results.
Oncology Nurses’ Role in Managing HSRs
Nurses must be aware of HSR symptoms and their expected timing so that they can promptly intervene if HSRs occur. Standard nursing care plans should include stopping oxaliplatin and starting normal saline, administering medications (e.g., dexamethasone, diphenhydramine, famotidine, epinephrine for anaphylaxis), taking vital signs, obtaining a 12-lead echocardiogram for chest pain, and notifying the primary oncology provider. Nurses also need to educate patients about the reaction and help manage any anxiety.
For more information about oxaliplatin HSRs and the opportunity to earn 0.5 CNE contact hours and ILNA points (free for ONS members), refer to the full article by Rogers et al.
Questions regarding the information presented in this article should be directed to the Clinical Journal of Oncology Nursing editor at CJONEditor@ons.org. Photocopying of this article for educational purposes and group discussion is permitted.