





Ophelia is a 42-year-old patient who has been diagnosed with triple-negative breast cancer (TNBC). She completed neoadjuvant chemotherapy with dose-dense doxorubicin and cyclophosphamide, followed by paclitaxel and carboplatin. Her postsurgical pathology shows residual disease in the tumor (3.5 cm down from 4 cm) and 12 out of 18 lymph nodes that are positive for cancer. Ophelia tells you that she is very discouraged and expected a better treatment outcome.
What Would You Do?
An understanding of breast cancer molecular subtypes (luminal A, luminal B, HER2-enriched, and basal-like) helps clinicians guide treatment and predict response to therapy. Identifying a patient’s TNBC subtype allows providers to personalize treatment options and identify potential targeted therapies (see sidebar).
The basal-like 1 (BL1) subtype has the highest rate of pathologic complete response because of its increased sensitivity to platinum-based chemotherapy. Poly adenosine diphosphate-ribose polymerase (PARP) enzyme inhibitors are the targeted therapy of choice for BL1-classified tumors with BRCA1 or BRCA2 variants or BRCA-likeness. Growth factor signaling pathways are showing promise in the basal-like 2 (BL2) group.
Inhibiting immune checkpoints like CDK4/6 and PI3K is another potential target for specific TNBC subtypes. Androgen blockade is being considered in the luminal androgen receptor subtype. Given TNBC’s heterogeneity, identifying its molecular subtypes expands the opportunity for personalized treatment.
You tell Ophelia that treatment possibilities for TNBC are increasing. You encourage her to talk with her oncologist about her next phase of treatment and the possibility for clinical trials.
Ophelia is interested in connecting with other people with TNBC, so you suggest the Triple-Negative Breast Cancer Foundation (tnbcfoundation.org), which has resources and a forum for patients with the disease.
TNBC Molecular Subtypes
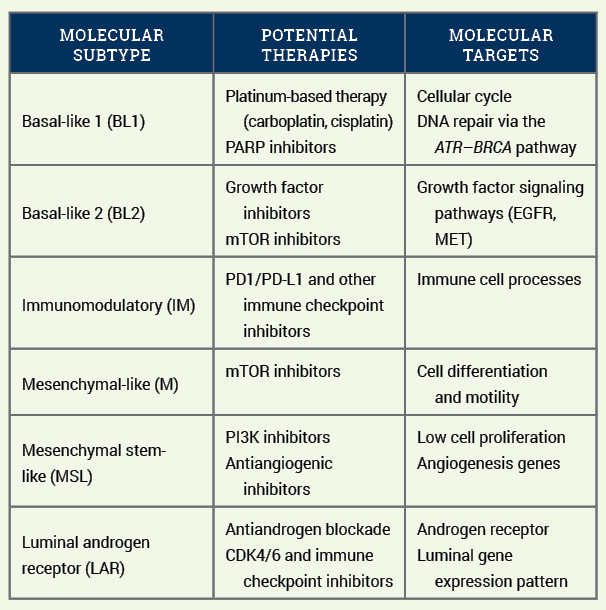
Note. Based on information from Lee et al.